
As a kinesiologist, I do not determine cause of pain. However, I can comfortably work around painful regions. The shoulder mobility screen within the FMS in interesting; it quantifies range of motion (ROM), however, it does not seem to determine stability. Therefore, an individual can score high (i.e., “3” left shoulder and “3” right shoulder) yet still have poorly controlled scapulohumeral motions. Of course, the other screens can identify shoulder stability (I.e., trunk stability push-up / rotary stability) if you look for it.

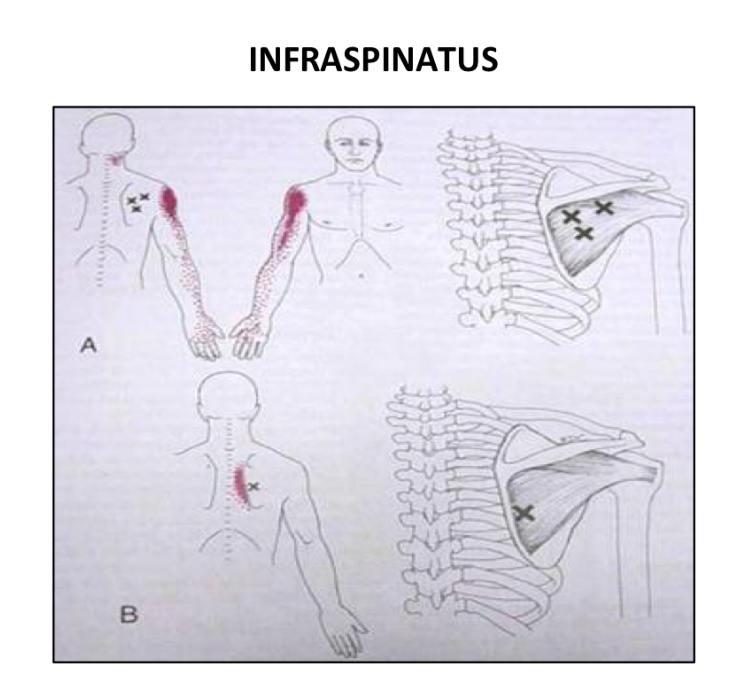
The impingement test is good as it helps the exercise professional determine if there are issues in, and around, the glenohumeral regions. However, pain around the shoulder can come from other sources as well. One of many examples, are myofascial trigger points within the rotator cuff muscles (Bron, Dommerholt, Stegenga, Wensing, & Oostendorp, 2011). Bron et al. (2011) noted that shoulder pain could emanate from the infraspinatus if it has a myofascial trigger point (MTP). Below is a picture outlining regions along the shoulder and arm, that an infraspinatus MTP can affect distally.
After my consultations and movement screens, I generally move clients through some mode of self-myofascial release (SMR), beginning with the bottoms of the feet, all of the way up to the bottom of the neck. I generally cover: calves, front thighs, hips, lowback, upper back (including rotator cuffs). As part of the warm-up, I include all of the aforementioned regions, if tender.
References
Bron, C., Dommerholt, J., Stegenga, B., Wensing, M., & Oostendorp, R. A. B. (2011). High prevalence of shoulder girdle muscles with myofascial trigger points in patients with shoulder pain. BMC Musculoskeletal Disorders, 12, 139.
-Michael McIsaac