Shoulder pain and dysfunction are common with a 6–11% prevalence in the under-fifties and 16–25% in the elderly (Alizadehkhaiyat, Fisher, Kemp, Vishwanathan, & Frostick, 2011). Alizadehkhaiyat et al. (2011) submitted that the infraspinatus (ISP) and supraspinatus (SSP), specifically, have key multifunctional roles to shoulder stability and movement. It is the contention of Alizadehkhaiyat et al. (2011) that the aforementioned rotator cuff muscles share a pertinent relationship with grip, and grip strength. Shoulder pain and impingement (i.e., organismic constraints) are generally caused, and aggravated by, overhead tasks and repetitive shoulder motions (Alizadehkhaiyat et al., 2011). Discovering methods that reduce degrees of freedom in the shoulder, while strengthening the rotator cuff muscles, are therefore relevant considerations during early stages of rehabilitation. The following will explore conservative, yet effective strategies, for rotator cuff strengthening using grip strength (i.e., task constraint) protocols.
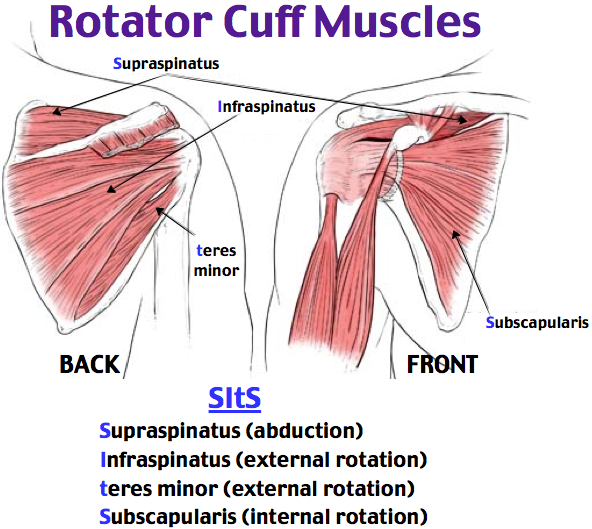
The glenohumeral joint is the most mobile joint in the body; many muscles contribute to both its mobility and stability during static and dynamic motions. Alizadehkhaiyat et al. (2011) noted that although many muscles contribute to shoulder function, the ISP and SSP play significant roles; the SSP is an abductor of the shoulder and plays a key role in external rotation. The ISP is the primary external rotator of the glenohumeral joint and contributes to arm abduction, in addition to assisting in stabilization during dynamic shoulder motions (Alizadehkhaiyat et al., 2011). What is also understood is that forceful gripping activates EMG activity of both rotator cuffs, with and without, motion at the shoulder joint. Moreover, activation of the rotator cuffs is higher during gripping motions than from inducing motion about the shoulder joint (Alizadehkhaiyat et al., 2011).

All subjects in the experiment of Alizadehkhaiyat et al. (2011) were in a seated position with elbows by the side and flexed at 90°. Additionally, all hand grip strength tests were performed at 50% of maximal voluntary contraction (MVC). Knowledge of methods indicates that rotator cuff activation occurs not only from a 100% MVC. Additionally, activation and fatigue of the rotator cuffs have occurred as low as 5% MVC (Alizadehkhaiyat et al., 2011). Such information indicates the close relationship of the IFP and SSP EMG activity to various percentages of MVC. When considering the researchers restricted the DOF while performing their experiment, it may indicate that increasing the DOF while inducing grip strength during early stages of rehabilitation may be a premature protocol.

The shoulder is a joint, which demands a large ROM while exhibiting simultaneous demonstrations of static and dynamic stability. Exercise regressions and progressions are key paradigms in the fields of rehabilitation and performance enhancement; determining placement of an individual along the aforementioned spectrum is key. Knowledge of rotator cuff activation patterns to seemingly insignificant percentages of maximal grip strength is central to exercise programming; such awareness helps substantiate how apparently conservative approaches (i.e., gripping tasks with no motion at the shoulder) still provide adequate neuromuscular input to the rotator cuffs and shoulder joint.
References
Alizadehkhaiyat, O., Fisher, A.C., Kemp, G.J., Vishwanathan, K., & Frostick, S.P. (2011). Shoulder muscle activation and fatigue during a controlled forceful hand grip task. Journal of Electromyography and Kinesiology, 21(3), 478-482.
-Michael McIsaac